Perfusion Lung Imaging
- Radiopharmaceutical used is99mTcMAA
- Size requirements
- 10 - 90 microns (90%)
- < 150 microns (10%)
- Capillary size = 7 - 8 microns
- Blocks the lower arteriole level of lungs
- The range of blocking the arterioles is between 1 to 1,000 to 1 to 10,000
- What would happen if we blocked all the arterioles?

- Regarding disease - if a blood clot(s), pulmonary embolus/i (PE) is several hundred microns in size and if radioactive particles are blocked from passing, what would you expect the PE to look like? Hot or Cold area?
- Technical considerations when administering 99mTcMAA
- When administering an IV injection - do not flush the syringe with the patient's blood

- May cause the particles to clump with the RBCs creating small hot spots in the lung because the RBCs may clump with the particles
- When administering an IV injection - the patient should be in the supine position
- If the patient is sitting upright when the IV is administered - MAA may tend to gravitate towards the at the base of the lungs
Perfusion Lung Procedure
- Administer 4 - 5 mCi of 99mTcMAA IV, while the patient is in the supine position
- Tell the patient to take several deep breaths during and after the injection
- Set Matrix size at 256 by 256
- Each image should be acquired for 500 to 1000k images or 5 minutes
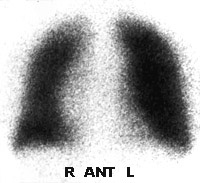
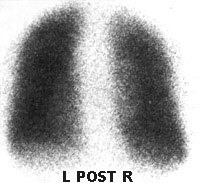
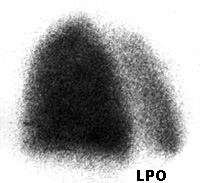
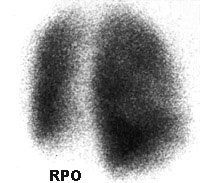
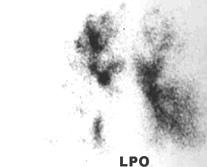
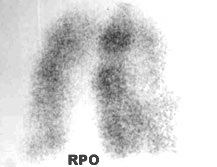
- Take ANT, POST, LPO, RPO images. Other images that are less important, but may also be taken include: LAO, RAO, L-LAT, and R-LAT
- All perfusion images must match the same angles taken with the ventilation image if 99mTcDTPA (aerosol) is used
- A chest x-ray must accompany the procedure. If it is more than 24 hours old, then a new x-ray must be taken.
Examples of the images shown below:
- Normal Perfusion Lung Scan injected with MAA
- Aerosol Ventilation Lung Scan with PE
- Aerosol ventilation Lung Scan with COPD
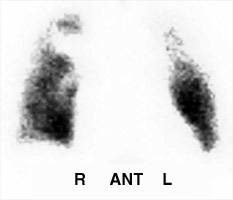
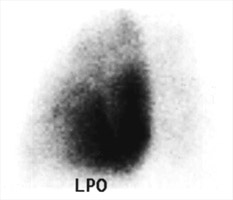
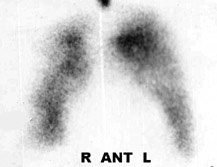
The first set of images is an example of a normal perfusion lung scan.
Note the perfusion of the MAA particles are evenly distributed throughout the lung. Keyword - homogeneity - normal perfusion.
Along with a perfusion lung scan, a ventilation lung scan must also be completed which is reviewed in the next lecture. To completely appreciate a V/Q lung scan one must also include the ventilation lung scan.
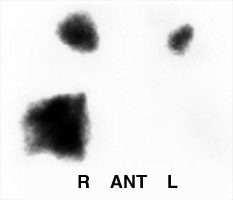
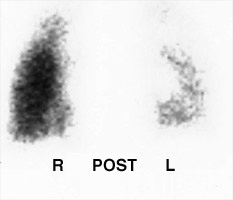
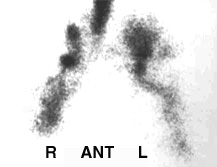
Another example shows a V/Q Lung procedure with a high probability of PE. The patient is injected with MAA for the perfusion portion of the exam and then administered radio-aerosol. The patient inhales 99mTcDTPA through a nebulizer that administered small radioactive droplets which stick to the mucosal lining of the lungs (see next lecture). In the perfusion portion of the exam, 99mTcMAA shows a mismatch defect! This is characteristic of PE. MAA is cold and with PE and hot with DTPA.
 Ventilation
Ventilation
|
 Perfusion
Perfusion
|
 Ventilation
Ventilation
|
 Perfusion
Perfusion
|
 Ventilation
Ventilation
|
 Perfusion
Perfusion
|
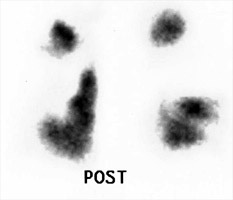
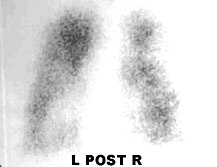
In our last example 99mTcDTPA aerosol with 99mMAA. In this case, the patient with COPD. In this type of disease the "water" droplets adhere or clump in areas where the lung contains an excessive amounts of mucus and/or fluid. Characteristic for COPD, aerosol "clumps" and the droplets cannot continue along that same airspace. Depending on how badly damaged the lung parenchyma is MAA may also not perfusion into the same area. This means that MAA and DTPA may have a matched, cold, defect.,
 Ventilation
Ventilation
|
 Perfusion
Perfusion
|
 Ventilation
Ventilation
|
 Perfusion
Perfusion
|
 Ventilation
Ventilation
|
Perfusion
|
 Ventilation
Ventilation
|
 Perfusion
Perfusion
|
Consider the above images with the following abnormalities: PE, COPD ("hot grapes"), Central deposition of activity in the main stem bronchi (DTPA).
Lung Perfusion Exam
Return to the beginning of the document
Return to the Table of Contents