Nuclear Cardiology - Part 1
- Cardiac Perfusion Agents -radiopharmaceutical perfuses myocardial tissue with the greatest concentration found in the left ventricle (LV)
- 201Tl - Thallium
- T1/2 = 74 hours
- keV = 80
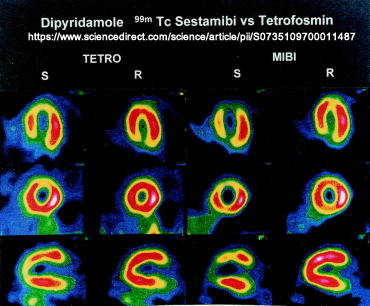
- 99m Tc-sestamibi (Cardiolite)
- 99mTc-tetrofosmin (Myoview)
- Pathophysiology
- Blood flows through the coronary arteries to determine if there is normal blood flow, (no occlusion) or some form of particle/complete blockage.
- When a radiotracer is injected into the bloodstream it flows to the coronary arteries where it will perfuse into the tissue but the amount of uptake depends on normal flow, partial occlusions, and/or myocardial infarct. Uptake of the radiotracer indicates viable myocardial tissue in the left ventricle (LV)
- In general, nuclear medicine examines the blood distribution and cardiac tissue viability in the LV. Why is assessing the left ventricle so important?
- Stress-induced ischemia (partial blockage)
- Ischemia occurs when there is a partial blockage in the coronary arteries causing reduced blood flow in the affected area
- Stress-induced ischemia is a condition that occurs when a partial blockage causes reduced blood to the coronary arteries. Usually, this is demonstrated when the heart is exercising
- Angina or chest pain may occur when the patient is being stressed which is caused to by reduced blood flow and the demand for more oxygen
- Myocardial infarction
- Lack of blood flow to the area
- It contains scar tissue. No viable myocardial tissue is seen
- When a radiotracer is injected, no activity is seen in the affected area/wall of the myocardium on stress or rest
- Types of radiopharmaceuticals
- 201Tl
- Is blood flow-dependent
- Myocardial tissue mistakes Tl for K. Hence Tl is an analog of K
- Details about this tracer and the acquisition protocol will be covered later when we will cover nuclear cardiology in CLRS 318
- 99mTc-sestamibi and 99mTc-tetrofosmin
- Is blood flow-dependent, and in this aspect, it is similar to thallium
- Sestamibi/tetrofosmin has great affinity for cells that have a high concentration of mitochondria
- Sestamibi/tetrofosmin concentrates in the myocardium because of increased mitochondria in these types of cells
- Administration of these tracers usually starts with the resting dose, it is injected and imaging occurs between 30 to 60 minutes after the injection
- The route of excretion for sestamibi includes the hepatobiliary system. Is background activity a concern? - Link
- A fatty meal or cold water may be given to facilitate washout from the hepatobiliary tree
- After the resting images are completed, the patient is stressed on a treadmill and a second dose of 99mTc-Sestamibi is injected; imaging occurs between 30 to 60 minutes post-dose
- Fatty meal or cold water may be given
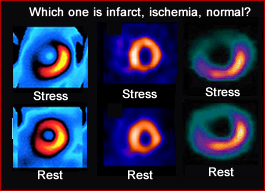
- Ischemia is seen when there is uptake of the tracer in rest but not in stress
- Infarct is seen when there is no tracer uptake in stress or rest
- In general
- Normal uptake in stress and rest = normal myocardial function
- Lack of uptake in stress, but uptake in rest = ischemia
- Lack of uptake in stress and rest = infarct
- It is imperative to get both stress and rest procedures for correlation and any possible cardiac disease
- During the stress portion of the exam, a treadmill is used to stress the patient
- Prior to the stress dose injection the patient must reach an 85% maximum level by applying the heart rate based and the patient's age
- Formula - (220 - patient age) x 0.85 = 85% maximum heart rate
- Exercising the patient with a treadmill (Most clinics use "Bruce protocol")
- Prior to the exercise procedure, the patient is attached to a 12-lead EKG for heart monitoring
- The treadmill starts with a slight elevation at a slow walk
- Every three minutes, the treadmill increases in speed and angle
- At the patient's 85% heart rate or greater, the radiopharmaceutical is injected
- Post injection the patient is exercised for one more minute
- Post-exercise the patient is monitored with the EKG
- Imaging occurs within the hour after exercise
- What comes first? Stress or rest imaging?
Note the difference!
- Sestamibi/tetrofosmin - Rest is done first, followed by the stress procedure.
- Note - Two important points: 1) Stress and rest have the same energy peaks and 2) The stress dose should be at least 3x the activity of the rest dose. Remember lung ventilation/perfusion?
- Pharmacological stress
- If the patient cannot reach a maximum level of stress, then certain drugs may be administered so that the same type of hemodynamics are achieved with blood flow to the coronary arteries
- Pharmacological test causing vasodilation via regadenoson/Lexiscan or adenosine
- Administered IV while the patient is in the supine position
- Lexiscan causes vasodilation in the coronary arteries
- Gives similar results why the patient exercises on a treadmill. Why is this a true statement
- Patients must discontinue Xanthine medication
- If the patient has a reaction to these vasodilators then aminophylline can be administered
- Other pharmaceuticals can be used to stress the patient and will be covered in CLRS 318
- Imaging the myocardium with 99mTc-Sestamibi and 99mTc-Tetrofosmin
- One day protocol
- Inject IV 7 to 10 mCi for the rest procedure
- Wait 30 to 60 minutes post dose before imaging
- May give the patient a fatty meal before imaging
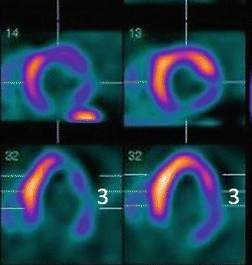
- Imaging is usually acquired in a SPECT format
- Imaging may also include a gated left ventricle to evaluate wall motion (refer to the MUGA lecture for details on gating)
- After the rest images are completed, the exercise test will be initiated
- Stress injection and acquisition
- Monitoring the patient with a 12-lead EKG, exercise the patient to 85% or greater level
- At peak exercise inject IV, 22 to 30 mCi and continue exercise for one more minute (remember 3 to 1 ratio?)
- Wait 30 to 60 minutes post-dose before imaging
- A fatty meal may be given prior to the SPECT acquisition
- Imaging is usually includes "gating" to assess left ventricle wall motion - See MUGA (lecture 3)
- Two-day protocol - To be discussed in the future
- Components of a successful cardiac stress test are essential and should be identified
- How is the patient going to be stressed?
- What type of radiotracer are you going to administer?
- How long between the injection(s) and the scan?
- Know the pharmacological agents and adjust accordingly
You Tube Video - "Nuclear Scan" http://www.youtube.com/watch?v=yJk_NN4Cn4U&feature=related
99mTc-sestamibi/tetrofosmin Procedure
Nuclear Cardiology Part II - SPECT Imaging Lecture
Return to the beginning of the document
Return to the Table of Contents
6/22