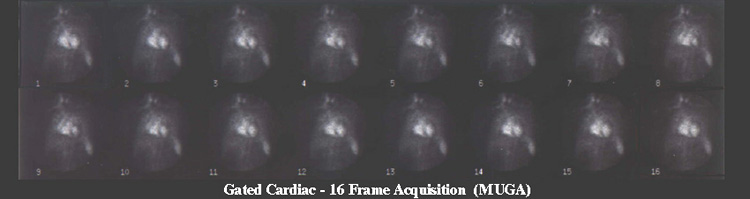
- Multigated acquisition - May be referred to as a MUGA or CINE, and it is a planar acquisition of the LV showing myocardial contraction
- SPECT perfusion can also be gated, usually done only on the stress images. The exception is MCV where stress and rest images are gated. The process of gating a SPECT is similar to the MUGA imaging and will be reviewed in detail next Spring
- MUGA acquisition and the gating process will be discussed now
- By labeling the red cells with 99mTc and re-injecting it into the patient, gated myocardium data can be acquired as blood flows through the left ventricle of the heart
- As the muscles of the LV contact, it pushes the labeled red cells out the aorta, and by gating, we can evaluate the function of musculature contraction
- In vivo RBC labeling - covered in the Spring
- In vitro RBC labeling (most common)
- 2 - 3 ml of blood is removed from the patient and labeled in vitro
- The kit required for this procedure is called "Ultra Tag"
- Refer to the package insert for labeling
- Once the blood is labeled, it is then re-injected, and images are acquired
- Modified In Vitro RBC labeling - hold for future discussion
- The key ingredients in labeling RBCs
- Stannous ion enters the red cell with the role of reducing 99mTcO4- locking the radioisotope into the cell
- Once the blood is labeled the; acquisition may begin
- First, look at the figure above, an electrocardiogram (EKG)
- The following parts of the EKG wave or electrical activity of the myocardium are identified:
- Three leads are attached to the patient pick up the R wave so R to R intervals can be recorded. The R wave is critical and allows for cardiac gating
- How is the heart gated?
- The EKG signal determines the R wave and the computer sets up a series of gates/frames
- From the above, diagram notice how the R to R interval is subdivided into five sections
- Each section, frame, or gate is considered as a segment of time where counts are collected and stored
- Each time the R wave is recorded, the acquisition resets itself to the first frame and data is recollected storing the counts from eahc R to R interval
- The acquisition continues until enough counts are collected within each frame
- Images above the EKG wave represent the data collected in each frame
- A resting image usually contains about 400 beats or R waves. The amount of counts in 400 R's is usually enough to give adequate resolution
- Images can then be played back in a dynamic cine mode to evaluate myocardial wall motility (see image below - "Displaying the MUGA")
- Displaying the wall motion
- Images show wall motion of the heart, however, in reality you are actually seeing labeled RBCs moving in and out of the heart chambers
- There are four types of wall motion to consider:
- Angles of the LV that are acquired that are imaged
- ANT
- RAO at 10 to 15 degrees
- LAO 30 - 45% (look for the angle of best separation of the LV)
- Steep LAO or LEFT LAT
- Examples of three different angles acquired in a MUGA
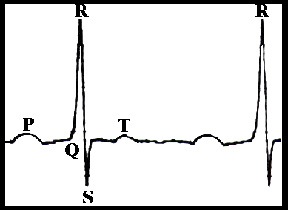
P - signal for sinus node impulse to depolarize the atria
QRS complex - electrical depolarization and contraction of the ventricles
P - recovery phase of the ventricles relaxes the contraction

Note: For demonstration purposes only five gates were used in the above diagram. Usually, the amount of gates is between 16 to 32
Normal contractility of all walls
Hypokinesis - one wall or section is moving slower than the rest
Akinesis - one wall or section is not moving at all when compared to the rest
Dyskinesis - one wall or section is moving in the opposite direction to the other

- All angles are played back s in a dynamic format
- Images can also be displayed in static mode (see the above)
- Images can be filtered to improve image quality (discussed next semester)
- Results of acquisition allow for the calculation of left ventricle ejection fraction (EF)
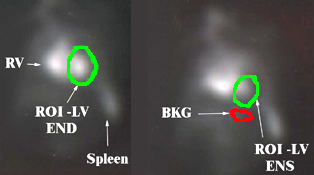
- From the images being displayed above, a region of interest is drawn around the LV
- Depending on how automated the computer software is, it may or may not be required to draw the initial ROI around the LV
- The first frame usually represents the end-diastolic (END), which contains the maximum amount of counts
- The computer will then calculate the activity of the LV for each frame
- The computer will find the frame with the least amount of counts (within the ROI) and define it as end-systolic (ENS)
- Finally, the computer will allow the user to confirm the ROI for BKG
- BKG is subtracted from each frame and then the ejection fraction formula is applied
- This generates a percent ejection fraction and an ejection fraction curve
- If necessary, any or all ROI(s) can be redrawn should the observer disagree with the automated ROI locations
- The above image shows ROIs drawn over the LV at END, ENS, and BKG
- The computer will also display an ejection fraction curve as noted below
![]()
- Above is an ejection fraction curve
- Usually, a MUGA study only involves resting images with the following angle imaged: ANT, RAO at 10 to 15 degrees, LAO 30 - 45%, and Steep LAO or LEFT LAT
- Stress gated cardiac procedure will be covered next Spring