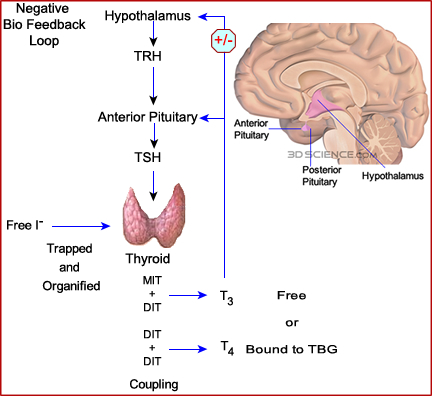
Radiopharmaceutical used for thyroid uptake and/or scan
Radiopharmaceutical |
123I |
131I |
99mTcO4- |
Physiology |
Trapped/organified |
Trapped/organified |
Trapped |
Gamma/beta |
Gamma |
Gamma/beta |
Gamma |
Dosimetry |
Low |
High |
Low |
T1/2 |
13 hours |
8 days |
6.02 hours |
KeV |
159 |
364 |
140 |
Uptake/image |
Both |
Both |
Image only |
Therapy |
No |
Yes |
No |
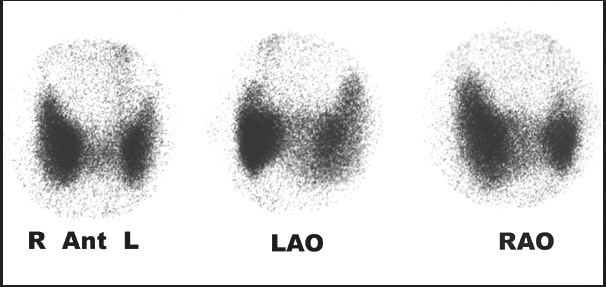
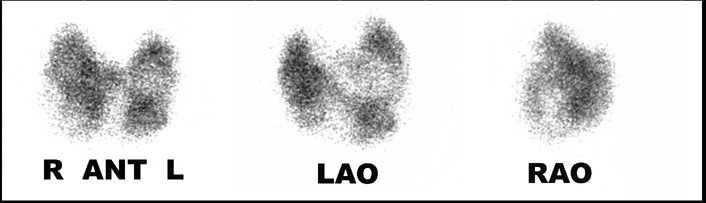
This is an example of a normal thyroid scan. Three views are taken ANT, RAO, and LAO. No marker image is seen, however, suggested. The marker should be placed at the sternal notch and on any/all nodules noted from thyroid palpation
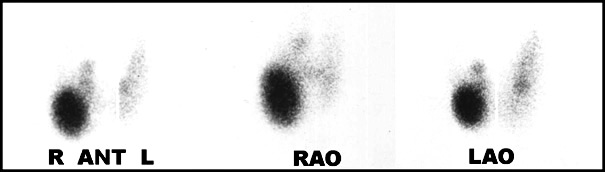
Before we look at disease from an imaging standpoint, what does a thyroid goiter look like?

Thyroid Uptake Procedure
Thyroid Scan with 123I
Return to the Beginning of the Document
Return to the Table of Contents
{kind=link}