- Initial distribution with 201Tl
- Dependent on regional blood flow and the extraction fraction
- 201Tl has an 87% of normal flow rates
- In general, animal data shows a linear relationship with uptake and blood flow (except for high end flow). As you increase the stress, you increase flow, and you increase tracer uptake
- At low flow rates uptake is extremely high while at high flow rates extraction reduces (how might this effect uptake)
|
Low flow rates = high extraction fraction
High flow rates = low extraction fraction |
- Increased stress levels with increased O2 demand does not degrade thallium uptake
- Roll off maybe another issue
- Pharmacological stress agents may cause 201Tl to "roll off" which is do to excess flow rate from the agent
- However, data indicates improved accuracy when low level exercise and pharmacological stress are combined (interesting)
- Reduced O2 levels may reduce the extraction fraction (do you want this to happen in an MPI study?)

- Oxidative phosphorylations may reduce or inhibit 201Tl uptake. This is where the heart burns fatty acids
- Glycolytic pathways may inhibit 201Tl uptake, which is the breakdown of carbohydrate via phosphate derivatives, which result in the production of lactic acid. There is an FDG connection to this as well.
- GachonP analyzed oxidative phosphorylation in cultures that had heart tissue and concluded that there is an apparent indirect reduced uptake with thallium 1
- Additional literature searches were inconclusive
- Summary - Administration of 201Tl is effected by exercise and vasodilation that will identify normal/abnormal myocardial wall uptake
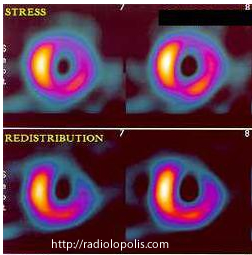
Redistribution
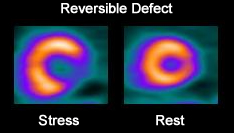
- In ischemic patients, myocardial defects seen on stress fill in at redistribution/rest. The initial lack of uptake is a direct result of vasoconstriction (partial occlusion of a coronary artery)
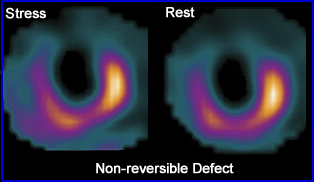
- Infarct will appear cold in both sets of images (stress and redistribution)
- Redistribution results because of the dynamic nature of an ischemic area
- Even rest images alone show redistribution in patient with severely stenotic coronary arteries
- Thallium is King when it comes to finding infarct and ischemia
- Why does it redistribute? This only occurs with 201Tl
- Systemic circulation occurs (>90%)
- The heart (~ 4%)
- Partial occlusion means reduced uptake of the radiotracer during stress
- As blood flow reduces (as patient returns to a resting state) those hypoperfused areas (partical occlusion) of the myocardium picks up thallium over time
- The exchange continue over time
- Proportional to cardiac out
- Perfusion = extraction fraction
- Blood is the mechanism of transport
- Systemic input and myocardium output
- Output = intrinsic myocardial washout rate
- Washout rate is also effected by blow flow, in that the level of occlusion relates to the rate of washout
- The difference between input and output effects the washout rate
- Equilibrium between blood flow and the myocardium eventually will result
- Biological T1/2 = 75 minutes
- The gradient
- Because of the increased blood flow during stress the "gradient" to the myocardial tissue is greater when compared to the resting state. For this reason, there is increased uptake of 201Tl during stress
- Apparently washout rates are not affected by different levels of stress
- Disappearance of thallium from the blood stream does affect the washout rate
- Relationship between normal hearts, redistribution and the filling in of ischemic areas is usually 2 - 4 hours
- Rest injection reaches equilibrium in ~2 hours
- Washout rates affect reversibility
- This reversibility may take up to 24 hours when partial occlusion is >90%. So why do a 24 hour delay?
- Sometimes up to 1 mCi is given 15 minutes before the redistribution images in order to avoid the 24 hour delay
- Post stress - glucose loading my reduce thallium uptake. How does this affect redistribution?
Myocardial Kinetics and Patterns of Defect
- Reversible - defect that initially lacks activity, but fills in at rest = ischemia
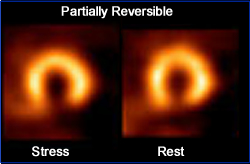
- Partially reversible - defect that initially lacks activity, but only partially fills in on delays = ischemia and infarct
- Non-reversible- defect lacks activity in both initially and delayed images = infarct
- Reversed redistribution - defect that has activity on rest images, but lacks activity in delays
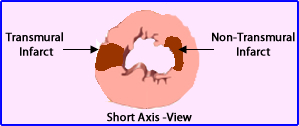
- Non-transmural myocardial infarct = reversed redistribution
- Transmural infarct = non-reversible defect
- Why should delayed imaging always be done? Should not all imaging center take a resting image?
- Here is an example of it
Return to the beginning of the document
Return to the Menu Page
1/20
1. Relationship between 201Tl uptake and oxidative metabolism in cultured myocardial cells, GachonP, et. al.