- T1/2
- Energy
- Redistribution
- Attenuation
- Wall motion
- Thrombolytic therapy - article
- What are the risks to this approach?
- How quickly does the heart tissue become necrotic after arterial occlusion?
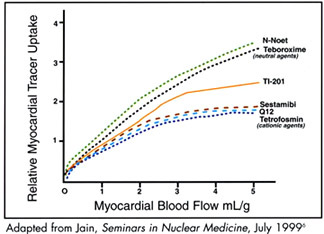
- Extraction Fraction
- Lipophilic monovalent cation
- Sestamibi adheres to the mitochondria via a negative transmembrane potential
- Sestamibi will only go to viable myocardial tissue via an adequate blood supply
- Two critical factors for uptake is
- Flow flow
- Viable myocardial tissue that contains mitochondria
- Further details link to this Article - "Technetium (99mTc) Sestamibi"
- Extraction fraction is less than 201Tl
- May overestimate myocardial scarring at high flow rates, which occurs during pharmacological stress test (can you explain why?)
- This agent undergoes minimal redistribution, about 20% within 20 to 60 minutes post dose
- Result may underestimate an ischemic defect, do to this redistribution (can you explain why?)
- To minimize the redistribution effect imaging should be started within 15 minutes post stress injection and the rest dose within 60 minutes post injection (why would you have to wait 60 minutes post rest before imaging?)
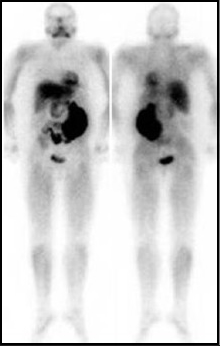
- Hepatic and bowel uptake (whole body distribution of sestamibi is seen above)
- Primary route of excretion is 33% from the hepatics (T1/2 = 30 minutes)
- Left lobe and gall bladder may interfere with imaging/processing
- Small bowel uptake may interfere with imaging/processing
- Furthermore, interference my draw counts away from the myocardium
- Following an MPI procedure a lung scan is completed on the patient 24 hrs later. Besides lung uptake, what else would you expect to see on a VQ scan?
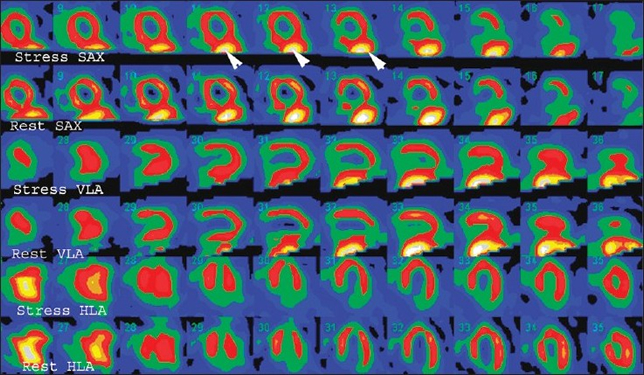
- High hepatic uptake may cause inferior wall defect(s) as seen above - like the image to enlarge
- Renal excretion = 25%
- Target organ is the upper large intestine
- Sensitivity = 90% and specificity = 80%
- Imaging and processing will be discussed later