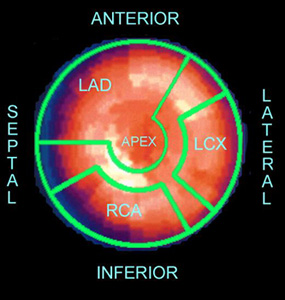
Coronary Arteries |
Anatomical Structure of the LV |
|
LAD - Left Anterior Descending |
Septal Wall |
|
LCX - Left Circumflex |
Anterior Wall |
|
RCA Right Coronary Artery |
Inferior Wall |
|
Lateral Wall |
17 Segment Polar Map
Analysis of the 17 Segment Polar Map |
|||||
1 - Basal Anterior |
LAD |
7 - Mid Anterior |
LAD |
13 - Apical Anterior |
LAD |
2 -Basal Anterior Septal |
LAD |
8 - Mid Anterior septal |
LAD |
14 - Apical Septal |
LAD |
3 - Basal Inferoseptal |
RCA |
9 - Mid Inferoseptal |
RCA |
15 -Apical Inferior |
RCA |
4 - Basal Inferior |
RCA |
10 - Mid Inferior |
RCA |
16 - Apical Inferior |
LCX |
5 - Basal Inferolateral |
LCX |
11 - Inferolateral |
LCX |
17 - Apex |
LAD |
6 - Basal Anterolateral |
LCX |
12 - Anterolateral |
LCX |
||
Finally a link for 3D display of myocardial blood flow distribution: http://www.yale.edu/imaging/anatomy/heart_sa_view/index.html